Browse by specialty
- Anesthesia and Perioperative
- Cardiology & Cardiovascular System
- Clinical Pharmacology
- Dermatology
- Diagnostic Imaging
- Emergency Medicine
- Endocrinology
- Ethical, Legal, and Organizational Medicine
- Family Medicine
- Gastroenterology
- General Surgery
- Geriatric Medicine
- Gynecology
- Haematology
- Infectious Disease
- Nephrology
- Neurology
- Neurosurgery
- Obstetrics
- Ophthalmology
- Orthopedics
- Otolaryngology
- Pediatrics
- Plastic Surgery
- Population and Community Health
- Psychiatry
- Respirology
- Rheumatology
- Urology
Rheumatology
Full-Colour Atlas
Splinter/linear hemorrhages
Linear hemorrhages, i.e. splinter hemorrhages, seen on the nails may be a clue to an underlying connective tissue disease, such as antiphospholipid antibody syndrome.
For an image, please see: https://ars.els-cdn.com/content/image/1-s2.0-S1571507805050099-gr4.jpg
Heberden’s nodes
Heberden’s nodes in the DIP-joints due to formation of bony nodules, a clinical sign seen in patients with osteoarthritis. More commonly seen than Bouchard’s nodes.

Case courtesy of Dr. Roberto Schubert, Radiopaedia.org, rID: 15934
Bouchard’s nodes
Bouchard’s nodes in the PIP-joints due to formation of bony nodules, a clinical sign seen in patients with osteoarthritis.

Case courtesy of Dr. Samir Benoudina, Radiopaedia.org, rID: 43417
Systemic Lupus Erythematosus – SLE
Prominent scaly fixed erythema, flat or raised over malar eminences, tending to spare nasolabial folds (“butterfly rash”).

Scleroderma
Sclerodactyly showing bilateral swelling, a shiny wax-like appearance, and tapering of the fingers. May also note digital ulcers, nailfold telangiectasia, and periarticular calcinosis. Flexion contractures present in advanced disease. (Courtesy Dr. A. Fam)

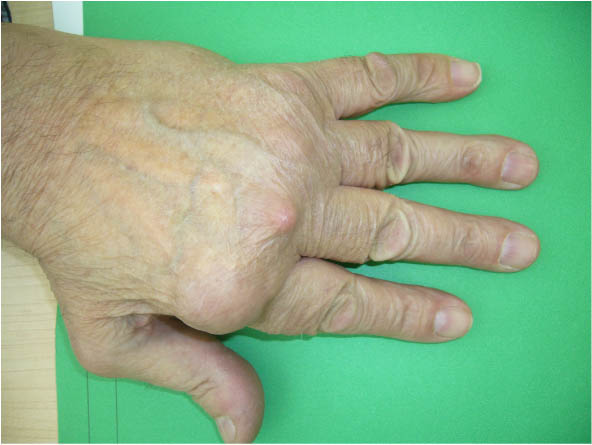
Rheumatoid Arthritis No. 2
Note subluxation of digits at the metacarpophalangeal (MCP) joints and rheumatoid nodules at 2nd and 3rd MCPs. (Courtesy of Dr. D. Jerome)
Rheumatoid Arthritis No. 1
Significant ulnar deviation of the digits, typical of rheumatoid arthritis.


Psoriatic Arthritis – Onycholysis
Onycholysis: Lifting of the nail starting at the distal end, seen in psoriatic arthritis. (Courtesy of Dr. D. Jerome)


Crytstals – Pseudogout
Acute Pseudogout (Calcium Pyrophosphate Dihydrate Crystals)
Polarized light microscopy showing calcium pyrophosphate dihydrate crystals. Note the positive bifringence (blue) of rhomboid-shaped crystals versus the needle-shaped and negatively birefringent (yellow) crystals of gout. (Courtesy of Dr. A. Fam)

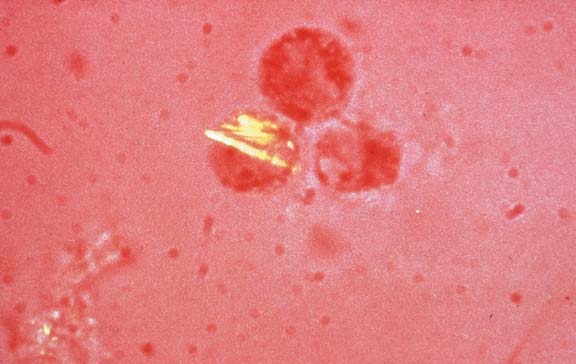
Crystals – Gout
Acute Gout (Monosodium Urate Crystals)
Polarized light microscopy showing monosodium urate crystals. Note the negative birefringence (yellow) of needle-shaped crystals versus the rhomboid-shaped and positively birefringent (blue) crystals of crystal pyrophosphate disease (CPPD). (Courtesy Dr. A. Fam)
Arthritis – Gout
Acute Gouty Arthritis
Classic inflammation resembling cellulitis of the first metatarsophalangeal (MTP) joint, referred to as podagra. The first MTP is the most common site of initial involvement. (Courtesy Dr. A. Fam)

Figure – 14
Left/right hand radiograph in a patient with osteoarthritis (OA), which shows joint space narrowing of the DIPs, osteophytes, and bone remodelling. These radiographic features are typical in mild to severe OA.

Case courtesy of Dr. Craig Hacking, Radiopaedia.org, rID: 69224
Figure – 9
Ring and long digit radiograph in a patient with psoriatic arthritis. There is loss of the tuft to the ring finger (arrow), so called acroosteolysis. The long finger shows soft tissue swelling (asterisk) with severe joint space loss and erosions at the proximal interphalangeal (PIP) joint. The bone density is increased involving the proximal and middle phalanx to the long finger (ivory phalanx) related to periostitis, a characteristic feature of psoriatic arthritis. (Courtesy of Dr. A. Donovan)

Figure – 8
Right foot radiograph in a patient with psoriatic arthritis. There is pencil-in-cup deformity involving the proximal interphalangeal (PIP) joint to the third toe (arrow). (Courtesy of Dr. A. Donovan)

Figure – 7
Left long finger radiograph in a patient with psoriatic arthritis and dactylitis. Note soft tissue swelling at the proximal interphalangeal (PIP) joint. Arrows show proliferative new bone formation. There is moderate joint space loss at the PIP joint. (Courtesy of Dr. A. Donovan)

Figure – 6
Left hand radiograph in a patient with rheumatoid arthritis shows extensive erosions at the distal radius, ulna, and carpus. Erosive changes are also seen at metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints. (Courtesy of Dr. A. Donovan)

Figure – 5
Right hand radiograph in a patient with advanced rheumatoid arthritis with erosions of the distal radius and ulnar styloid, as well as severe joint space loss with erosions throughout the carpus with soft tissue swelling. (Courtesy of Dr. A. Donovan)

Figure – 4
Right hand radiograph in a patient with advanced rheumatoid arthritis. There are extensive marginal erosions and ulnar subluxations at the metacarpophalangeal (MCP) joints. Erosions are also present at PIP joints. (Courtesy of Dr. A. Donovan)

Figure – 3
Right wrist radiograph in a patient with rheumatoid arthritis. The arrows show erosions at the ulnar styloid and distal radius. Asterisk shows additional erosions at the carpus. (Courtesy of Dr. A. Donovan)

Figure – 2
Left hip joint radiograph shows severe superior joint space narrowing, subchondral cysts, subchondral sclerosis and marginal osteophytes. These are radiographic hallmarks of osteoarthritis. (Courtesy of Dr. A. Donovan)

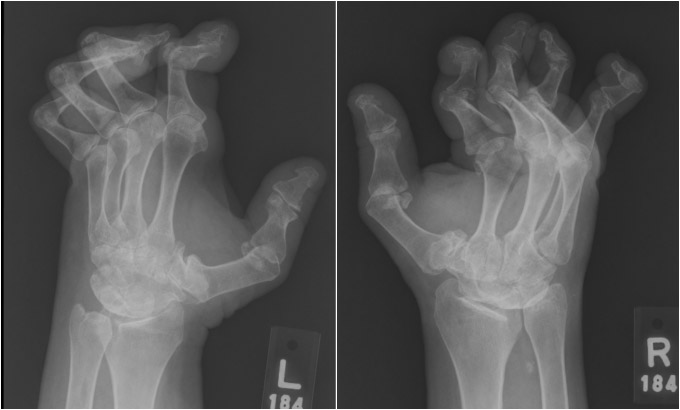
Figure – 13
Bilateral hands in a patient with lupus. Note finger flexion and extension deformities in the absence of erosions. (Courtesy of Dr. A. Donovan)