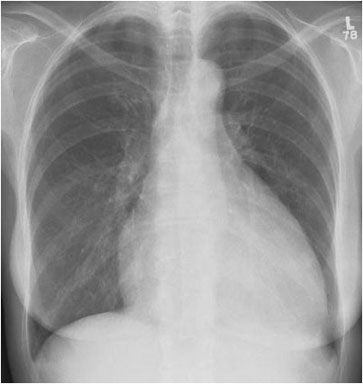
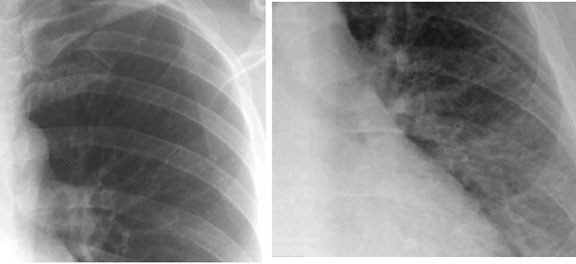
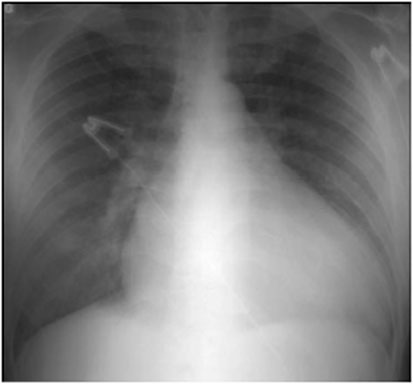
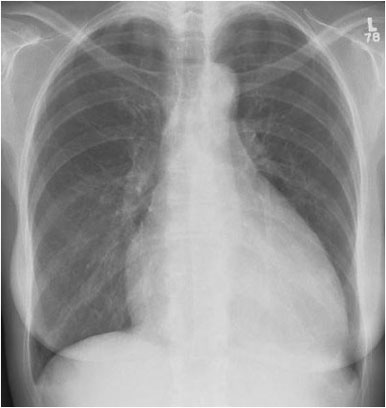
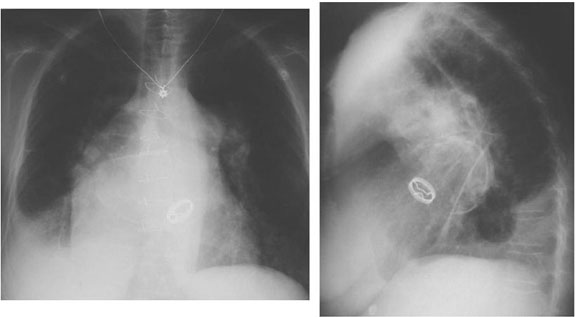
Right Ventricular Hypertrophy
Right ventricular hypertrophy is suggested by elevation of the cardiac apex from the diaphragm on this PA projection of a patient with rheumatic heart disease. The lateral view supports the diagnosis by demonstrating loss of the retrosternal airspace and increased contact of the right ventricle against the sternum. Also noted in this patient are mitral valve calcification, evidence of left atrial and pulmonary artery enlargement, and evidence of chronic congestive heart failure.