Figure – 12
Right wrist radiograph shows chondrocalcinosis involving the triangular fibrocartilage complex (arrow). (Courtesy of Dr. A. Donovan)

Study Smarter
Right wrist radiograph shows chondrocalcinosis involving the triangular fibrocartilage complex (arrow). (Courtesy of Dr. A. Donovan)
Elbow radiograph in a patient with gout. Note large soft tissue abnormality (arrows) superficial to the olecranon. This represents olecranon bursitis. In addition to gout, it can also be seen in patients with rheumatoid arthritis, or be related to trauma or infection. Bilateral olecranon bursitis is characteristic for gout. (Courtesy of Dr. A. Donovan)

Left toe radiograph shows well-marginated erosions with sclerotic margins (arrow) and overhanging edges (arrowheads) at the interphalangeal joint. The findings are consistent with gouty arthritis. Similar changes are seen at the first MTP joint. (Courtesy of Dr. A. Donovan)

Bilateral hand radiographs in a patient with osteoarthritis. There is moderate joint space loss at the first carpometacarpal (CMC) joints bilaterally (arrows) with subchondral sclerosis and cystic changes. The interphalangeal joints show similar changes. These are shown by the arrowhead. (Courtesy of Dr. A. Donovan)

Acute Pseudogout (Calcium Pyrophosphate Dihydrate Crystals)
Polarized light microscopy showing calcium pyrophosphate dihydrate crystals. Note the positive bifringence (blue) of rhomboid-shaped crystals versus the needle-shaped and negatively birefringent (yellow) crystals of gout. (Courtesy of Dr. A. Fam)

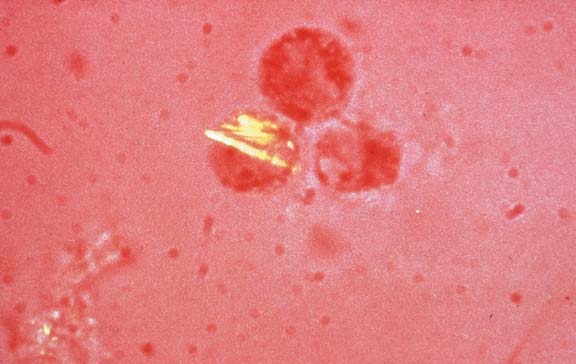
Acute Gout (Monosodium Urate Crystals)
Polarized light microscopy showing monosodium urate crystals. Note the negative birefringence (yellow) of needle-shaped crystals versus the rhomboid-shaped and positively birefringent (blue) crystals of crystal pyrophosphate disease (CPPD). (Courtesy Dr. A. Fam)
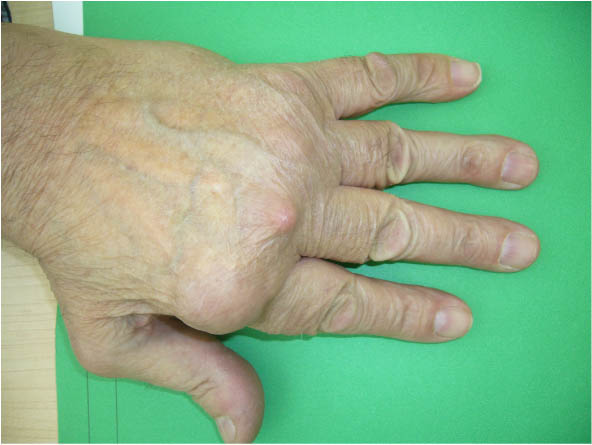
Acute Gouty Arthritis
Classic inflammation resembling cellulitis of the first metatarsophalangeal (MTP) joint, referred to as podagra. The first MTP is the most common site of initial involvement. (Courtesy Dr. A. Fam)

Prominent scaly fixed erythema, flat or raised over malar eminences, tending to spare nasolabial folds (“butterfly rash”).

Sclerodactyly showing bilateral swelling, a shiny wax-like appearance, and tapering of the fingers. May also note digital ulcers, nailfold telangiectasia, and periarticular calcinosis. Flexion contractures present in advanced disease. (Courtesy Dr. A. Fam)

Note subluxation of digits at the metacarpophalangeal (MCP) joints and rheumatoid nodules at 2nd and 3rd MCPs. (Courtesy of Dr. D. Jerome)