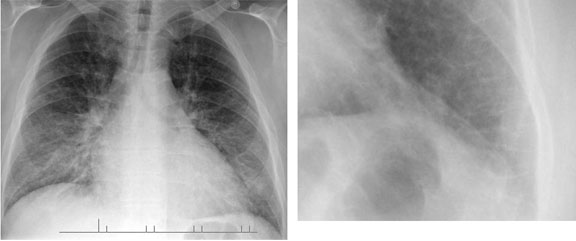
Pulmonary Nodules
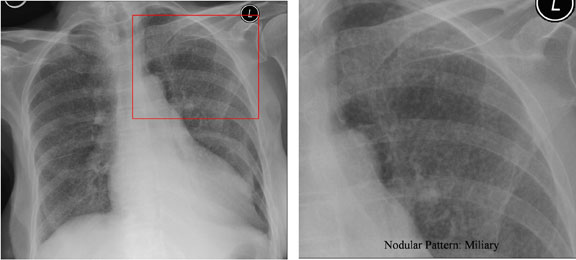
This image shows a pulmonary nodule in the right upper lung. Differential diagnosis of pulmonary nodules includes:
- Malignancy (primary or metastatic)
- Benign neoplasm: hamartoma, bronchial adenoma
- Granuloma
- Simulated: nipple, bone lesion, skin lesion, foreign body, artefact
Less common causes include:
- Abscess
- Infarct
- Loculated pleural effusion
- Organized pneumonia
- Sarcoidosis
- Cystis disease
- Vascular lesions