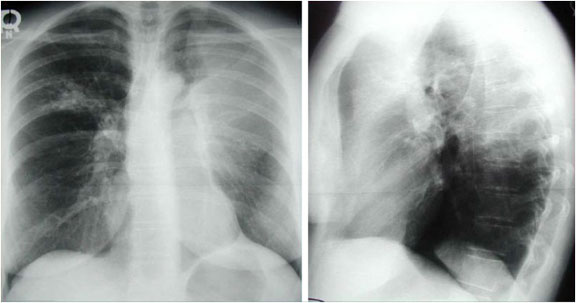
RUL Collapse
This patient has suffered complete collapse of the right upper lobe. Note the opaque, atelectatic right upper lobe projecting over the superior right hemithorax. This image is a good example of the “S-sign” of Golden: The displaced minor fissure resembles an inverted “S” in contour. The collapse is most likely due to a mass in the region of the right superior lobar bronchus. The collapsed right upper lobe also demonstrates the “silhouette” sign; in this case, the adjacent superior vena cava’s border is obscured by the right upper lobe. There is mild elevation of the right hemidiaphragm, consistent with atelectasis on the right. Although not convincingly seen here, other indirect signs such as hilar and mediastinal shift can also be present with atelectasis. Multiple surgical clips are noted in the region of the thoracic inlet.